The Perverse Nature of the Medical Profession

The natural business model of an army is to fight enemies, so any large army will find enemies to justify its existence. Similarly, the natural business model of a government bureaucracy is to solve problems of the population it “serves,” so a large bureaucracy should be expected to find or invent problems to justify its existence. In similar manners will a religion find or invent threats to our spirit or soul for which it is the solution, and government-subsidised scientists find or invent threats to humanity for which they are the solution.
Promoting behaviours and mindsets that serve to justify and perpetuate the industry is simply inherent to the way each of these industries operates. Those within an industry who do not play along quickly find themselves poor and ignored.
What is the business model of the medical profession? How does it naturally make its money, and what will that mean for the behaviour and worldview promoted by its members? Does the answer vary depending on what kind of ‘medic’ we are talking about, whether it be a pharmaceutical manufacturer, clinician, surgeon, pathologist, faith healer, or Ayurvedic?
The Mindset of the “Medicine” Business
From Hippocrates onwards, the simplest type of ‘medic’ has been an individual-to-individual supplier of healing services. This person supposedly has been guided by an ethical obligation to ‘do no harm.’ Arguably, the most revealing saying of Hippocrates is not the famous Oath, but rather the following: “It is more important to know what sort of person has a disease than to know what sort of disease a person has.”
This saying advises the healer to take a holistic view of an individual patient, which may sound good on the surface but is implicitly somewhat paternalistic. Hippocrates invites the medic to consider himself akin to a god or a Jesus-like figure, doing no harm and aspiring to high-level wisdom to sort out the deep problems of each individual patient he comes across.
In terms of mindset and marketing, medics have an economic incentive to see disease everywhere and to pretend to be able to fight it. An especially strong incentive exists to see chronic illness everywhere, since anything chronic enables a medic to find lifelong patients. Like any parasitical entity, the medic’s business is optimised when the host is not killed quickly but can be drained over time. The weakened host/patient is bled for as long as possible until the end is inevitable, at which point the bleeding ramps up to the maximum output level (essentially, what remains of the host is eaten). In biological terms, the most economically successful medic is a lifelong symbiont-parasite who becomes a detritivore at the end of a patient’s life.
Those in the medical profession may do some good early in the life of their hosts and at moments of acute injury or major illness during adulthood, as these actions promote survival of the host, which enables future parasitism. Beyond this, medics have a natural incentive to tell people that they are ill and in need of constant checkups and treatments, and to turn the final year of a patient’s life into a miserable enslavement to expensive ‘healing.’
Turning Disease into Dollars
In the US, the medical industry now accounts for 18% of GDP, meaning almost one in five dollars generated ends up in the pocket of a medic of some sort. In fairness, the US is the global outlier: it delivers a similar life expectancy (about 78) as both China and Cuba deliver to their people at about 20 times the per-capita cost spent by China, and 10 times that spent by Cuba. In China, only one in 20 dollars of GDP is spent on “medics,” broadly defined.
From these comparisons, we might deduce that only 1/10th of the health budget in the US buys actual health. So what is the other 90% spent on?
Consider the graph below, showing total medical costs by age category in the Netherlands, a country with many similar health-sector features as the US, and for which health expenditure is particularly well-documented. Expenses are non-negligible in every category, even for people in their late teens and 20s, due to constant checkups, diagnoses, and treatments. Expenditures have a mini-peak at birth, which over the decades has become an increasingly expensive hospital experience rather than a cheap midwife-assisted experience.
Spending soars in old age: expenses start to explode as one approaches 90, when the inevitable is nigh. For women (un)lucky enough to make it to the final age category in the graph, medical costs per person per year are close to 70,000 euros, equivalent to about twice the median yearly income. What we see on the graph is in line with the economic nature of the medical profession: 10% symbiont, 90% parasite, and detritivore.
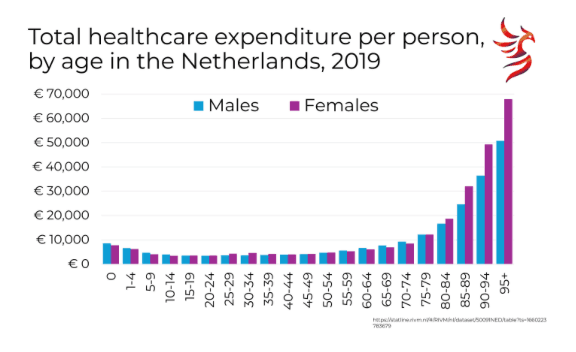
How much of this is spent on pharmaceuticals? The implication within MAHA circles that Big Pharma gets the lion’s share of the loot is contradicted by the reality that pharmaceutical companies of any size get only about 15% of the medical costs shown in the graph above. There are many more and varied parasites in the medical industry, beyond just the pharmaceutical companies.
Who else has their snouts in the trough?
The testing industry is a big beneficiary, with pathology labs and AI-testing kits going through an industrial revolution. Test enough, and you shall find medical problems even if they are not there. Men can even get a positive result on a pregnancy test, and not because they are actually women (or pregnant ones, for that matter). The same goes for tests for cancer and everything else. ‘False positives,’ in the jargon, lead to huge anxiety and unnecessary treatments, or in other words, bonus clients for the medical profession.
The perversity of the medical profession, as with the perversity of most parasitical professions, is clothed in morality and victim-blaming. Hippocrates himself started this tradition by insisting that illness revealed ‘sins against nature.’ The worse the illness, the worse the sin must have been! This trick works surprisingly well to prevent the patient from doubting the wisdom of the messiah-medic. During lockdown,s the ‘illness reveals sin’ motif was on display any time medics talked of ‘viral vectors,’ or of people ill with Covid not following the scriptures tightly enough (and consequently, now being punished with illness). ‘He must have met other people secretly.’ ‘She refused the mask.’ Pointing the finger of blame conveniently distracts those who might otherwise discover the blood on medics’ own hands.
Killing Both the Competition and the Patients through the Ages
What did the medical industry do with its competition over the ages? The time-tested strategy has been to dismiss the low-cost competition variously as witches, quacks, sorcerers, shamans, unethical, fringe, and satanic. Many thousands of midwives and herbologists were burned at the stake because they were in the way of well-paid doctors and their patient-victims. The medics murdered their competition, denounced their writings and remedies as heretical, and comprehensively threw them out of their club.
In the industrial age, medical killings became industrial, exemplified by the medically supervised gas chambers of the Nazis. In the ideology of that time, the murders that occurred in these chambers were curing the German lineage of a ‘scientifically validated’ illness. That repulsive ideology has its roots in the eugenics movement that was cooked up and promoted by anthropologists, medics, and other ‘scientists’ in the 19th century, and carried forward by the Nazis and many other groups. It is what gave us the lunatic asylums that delivered shock therapy and forced sterilisations to ‘the deplorables’ that continued into the 1950s in many countries. After the medical madness of WWII, non-German medics wrote the Nuremberg principles to denounce the actions of German medics, while themselves still advocating practices, like smoking, that kept people unhealthy.
The inherent moralising perversity of the medical profession has a long ancestry. As we showed in a recent paper with Jay Bhattacharya, the medical profession championed lockdowns for centuries because it brought in good business. In that paper, we quote Charles Maclean’s estimate in 1817 that nearly a million people per year had died unnecessarily since the 14th century because of the widespread practice of lockdowns (then typically called ‘quarantines’) championed by medical authorities. It was the Sanitarians who brought an end to the scam via the UK Public Health Act of 1848. It took another 50 years for the malpractice of lockdowns to end elsewhere in Europe, though it made a spectacular comeback all across the West five years ago.
Medical perversity was never truly conquered, though, even in the century following the Sanitarians’ heyday. As referred to above, doctors were among the last to admit that smoking was bad for people. Statisticians discovered this fact in the 1950s, and it took over a decade for the medical profession to agree, kicking and screaming. Until then, cigarette companies even used doctors in their advertising campaigns to assure the public that smoking was healthy. From the medics’ perspective, caving in and acknowledging that smoking was harmful to health would imply that they personally had done immense harm to populations for decades by telling them that smoking was good. Medics’ active pro-smoking stance alone must have killed tens of millions of people needlessly around the world, often after prolonged, painful, and expensive illnesses like lung cancer. We have never seen an apology from the medical profession for this unnecessary suffering and death that happened on their watch and at their bidding.
Sanjeev Sabhlok unearthed the shocking story that the convention of giving people harmful ‘vaccines’ goes back to the late 18th century, soon after which Sanitarian leader Charles Maclean, to his dismay, unearthed the ruse. Why did doctors do this? Because they could convince their patients to pay them for this dodgy service. In the longer run, the lack of correction against the vaccination ideology in the profession as a whole was due, in MacLean’s words, to “those obstinate Practitioners, who, because they have once been in error, according to their notions of consistency, deem it incumbent on them to remain always in error” (On the State of Vaccination in 1810, by Charles MacLean, Preface, page vii).
The lucrative vaccine gig grew into an industry whereby children in the US nowadays receive a recommended 36 shots (24 of them in the first year of life) by the age of 16, plus annual flu and Covid-19 vaccinations administered by individual doctors getting rich by injecting all of those chemicals, while telling themselves and their patients that it’s all for the good. Credible evidence now exists that large harms, including chronic problems like autism, are the likely result.
It is no wonder then that doctors were able to flip on a dime in early 2020 and tell their patients that going outside was a hazard, rather than totally necessary as a means of getting sunshine and exercise. It was completely in line with their historical inclinations to force harmful injections on their patients and to pretend that idiocies like wearing surgical masks at the grocery store and disinfecting surfaces in hazmat suits were useful, rather than inflicting harm.
Following their usual bad habits, medics ignored the importance of community and social life during the lockdowns. Real health and healing, much of which is supplied cheaply and effectively by strong families and supportive communities, have always been the natural enemies of the medical profession. What people find in functional and happy communities, not what they find in expensive and stress-laden hospitals, is what produces most human health. For this reason, strong communities are medics’ nemesis.
The fact that the most health-improving actions taken today are not funded by the ‘health’ budget line item is no accident. Clean water, regular garbage collection, basic sanitation infrastructure and services, safe roads, safe means of cooking, and plentiful food are cheap and have been provided by communities ever since the public health revolution of the mid-19th century. Once seen accurately as the very core of public health, these measures do not involve an individual hero saving an individual patient in need, and perhaps for that reason, they are now hidden in various non-‘health’ budgets. In fact, they form part of what the WHO is now perversely forcing poor countries to sacrifice in order to get more ‘life-saving medicine.’ The perversity of Western medicine is spreading globally, replacing actual health-improving investments.
But at Least I Have My ‘Alternative’ Doctor!
Is ‘functional medicine’ any better? Look no further than its ChatGPT description: functional medicine “focuses on identifying and addressing the root causes of illness, rather than just treating symptoms. It emphasizes the interconnectedness of body systems and how imbalances can lead to various health issues. By understanding a patient’s unique genetic, environmental, and lifestyle factors…”
What we see in this description is the ideology of yet another collection of ‘healers’ who remove the community’s role in supporting health and, like Hippocrates, place themselves in the chair of the all-knowing paternalist. There is again the implicit notion of sin here: ‘root causes’ and ‘imbalances’ imply the existence of a perfect state, known to the medic, that the ill patient has failed to achieve. Just like ‘normal medicine,’ functional medicine involves lots of tests on patients, with these tests designed to reveal a whole array of bodily and psychological imbalances requiring (of course!) lengthy and expensive treatment for which one involves the services of a functional medicine practitioner. Different mumbo-jumbo, but same basic business plan.
Indeed, any long-lived medical system (allopathic, Ayurvedic, traditional Chinese, etc.) involves a gatekept community of ‘healers’ working from the same basic mental structure: illness is portrayed as an individual problem caused by sin (imbalance, blockage, weakness, etc.) and solved at the individual level by the great healer, in the thrall of whose proscripts one is encouraged to live one’s whole life unless one wants to risk illness. In sum, perversity with a generous helping of paternalistic moralising.
Let us be clear: we are not saying that person-specific inputs such as nutrition and individual exercise have no role in health. Ensuring one gets enough vitamin D (read: sunshine) is important to support immunity, and moderate exercise is surely good for the body. Some medics give passing mention to such truths and some specialities (e.g., nutritional medicine) give them even more weight. Still, the lion’s share of time and money in most medical systems is spent on expensive treatments that are directed solely at individuals, particularly during the vulnerable period leading up to death, and have nothing to do with community functionality, sanitation, nutritional quality, or exercise levels.
It appears that healing systems that are not perverse die out, which we surmise is down to lack of funding and ineffective dissemination of their messages due to the above-mentioned name-calling by the successful medic-parasites. Unless you scare humans into costly compliance with your expensive mumbo-jumbo, you are ignored, and people instead flock to the next quack, whether in a big hospital or in the back alleys. The brief triumph of good policy initiated by the Sanitarians in 1848 was already largely eroded by the year 2000 and saw its last vestiges come crashing down in 2020.
And the Sham Goes on
How does the medical industry convince the general public of its noble intentions and magical healing powers? Simple: by actually saving people sometimes (think heart bypasses or fixing up broken legs) and otherwise providing the general public with appealing images of medical superheroes. Sexy young doctors intrepidly saving lives in TV series like House are the frontline image-builders, cutting Messianic figures that wield MRIs, intravenous chemical shots, and encyclopaedic knowledge of obscure diseases with hubris and swagger, all to the immense gratitude and awe of their patients. They project themselves in the same way that the armies in the Middle Ages projected the myth that knights were noble defenders of damsels in distress, rather than rapacious, sadistic maniacs terrorising the peasants.
For the devil to put on the face of the angel is an old trick that works in every century. People do love their heroes, even though there are almost none of them in real life. If someone were naïve enough to behave in real life like the TV doctor heroes behave, and hence take things like informed consent or ‘do no harm’ seriously in a crisis, they would soon be sued and cancelled. Just like Don Quixote de la Mancha was beaten up and ridiculed when he started to behave like the knights of the medieval stories, so too did the few ethical doctors get sidelined and smeared by their own profession during Covid times.
Is MAHA any better? We fervently hoped it would be part of the solution. We advised two years ago on what could be done if one focused on the small part of the medical industry that is useful, and more recently advised that MAHA could make a good start by tackling the medical-legal monopolies. That was February. Now things are looking markedly less good, despite recent progress in the mRNA saga.
Think of what MAHA now depicts as the promised land: a world of mass testing. RFK, Jr has a dream that we will all be wearing AI-powered health-testing watches in years to come. This embodies the myth of perfect testing all over again. It is the dream of all bureaucrats. Indeed, the whole notion of ‘evidence-based medicine’ is a bureaucrat’s dream. Worse, it’s the dream of the scientific bureaucrat who is going to oversee or perform all the required evaluation of evidence, plus the ensuing imposition upon society of the discovered scientific truth, sending his bill to that society, of course. The perfect scientist with his perfect test, telling the grateful patient, for a fee, what is wrong with his life and how he should live.
Consider for a moment what MAHA is not doing. Is MAHA breaking down the medical industry? Is it destroying the parasitical bureaucracy? Is it reducing testing rates; destroying the legal monopoly of ‘accepted medicine’ to supply healing; or empowering communities to provide healing via functional social life (as is done in Cuba)? No, MAHA is doing none of that. It is serving up old wine in new bottles, with well-paid white coats bringing salvation as the centrepiece. Same devil, new face.
We are also worried about the ‘evidence-based medicine’ mantra that MAHA is following. It sounds good, but in practice it appears to mean that the status quo will be protected until, bit by bit, it is ‘proven’ to be ineffective. That is not a recipe for getting very far with reforms. It is like using a nail clipper to prune a forest. No challenge to the hospitals or the insurance system can be mounted from that direction, nor can a switch be made to the Chinese or Cuban model. MAHA has proposed no policies on whose basis one could predict significantly reduced US health spending in the medium run, with a 2025 McKinsey report predicting robust increases in hospital spending and ‘specialty pharmacy.’ This makes MAHA and its mantras in danger of becoming no more than the latest veneer for the parasitical medical industry.
Our message to readers is blunt: nearly everyone in the medical profession, whether Ayurvedic, MAHA, traditional, AI-enhanced, pharma-led, faith-based, functional, or energy-based, has a strong economic incentive to be a pervert. Their incentives are to separate you from your community, convince you that you have problems you do not have, and sell you solutions you do not need that will make you worse off. They will make the end of your life a costly hell and, if you let them, the whole of your life an impoverishing compliance with their misdirections.
We offer you a simple rule of thumb: if someone is paid more than the average health-sector wage for ‘healing’ you (e.g., more than your local community nurse or midwife), then they are probably trying to do you harm, whether they know it consciously or not. There are exceptions, but like Don Quixote they are rare and usually shunned by their own colleagues. The only ones likely to truly help you are those who love you already and those rare humans willing to help others for almost nothing in return. If you have a major health problem, you will largely have to figure it out yourself and be prepared to be lied to and misled by nearly everyone along the way. The more highly paid and highly credentialled the medic, the more likely you should run in the opposite direction.
Look on the bright side, though. Refuse all the moralising and paternalising by the huge industry of perverse medics, and you can have a much freer and more enjoyable life than the compliant sheep are having. Plus, just think of all the money you will save!
-

Gigi Foster, Senior Scholar at Brownstone Institute, is a Professor of Economics at the University of New South Wales, Australia. Her research covers diverse fields including education, social influence, corruption, lab experiments, time use, behavioral economics, and Australian policy. She is co-author of The Great Covid Panic.
-
Paul Frijters, Senior Scholar at Brownstone Institute, is a Professor of Wellbeing Economics in the Department of Social Policy at the London School of Economics, UK. He specializes in applied micro-econometrics, including labor, happiness, and health economics Co-author of The Great Covid Panic.
-
Michael Baker has a BA (Economics) from the University of Western Australia. He is an independent economic consultant and freelance journalist with a background in policy research.